Sunday O Nduka1 ![]() ,
Chika Edebeatu1,
Chika P Isidienu1,
Kosisochi C Amorha2
,
Chika Edebeatu1,
Chika P Isidienu1,
Kosisochi C Amorha2
For correspondence:- Sunday Nduka Email: so.nduka@unizik.edu.ng Tel:+2348033644385
Received: 12 June 2016 Accepted: 20 June 2016 Published: 31 March 2017
Citation: Nduka SO, Edebeatu C, Isidienu CP, Amorha KC. Prescribing practices for pediatric out-patients: A case study of two teaching hospitals in Nigeria. Trop J Pharm Res 2017; 16(3):705-711 doi: 10.4314/tjpr.v16i3.28
© 2017 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: The objective of this study was to evaluate drug utilization pattern in the pediatric departments of two tertiary health facilities in Nigeria using WHO core prescribing indicators.
Methods: Using a cross-sectional retrospective study approach, prescriptions randomly selected for a period of 6 months from the pediatric out-patient departments of two tertiary hospitals: Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), Awka and Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi in South- Eastern Nigeria were assessed. Prescribing indicators as listed by WHO were calculated and analyzed using SPSS version 20.
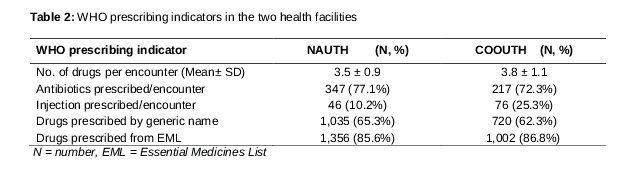
Results: A total of 750 prescriptions (450 from NAUTH and 300 from COOUTH) containing 2,739 drugs were assessed. The mean number of drugs prescribed per encounter (mean ± SD) at NAUTH was 3.5 ± 0.9 and 3.8 ± 1.1 in COOUTH. The percentage of antibiotics prescribed per encounter in COOUTH and NAUTH were 72.3 and 77.1 %, respectively, whereas drugs prescribed by generic names were 61.7 and 64.2 %, respectively. Injections prescribed per encounter were above acceptable range, and percentages of drugs prescribed from essential medicine lists in the two hospitals were > 85 %.
Conclusion: This study identified irrational use of antibiotics, polypharmacy, non-adherence to generic prescribing and high use of injections in both hospitals. The need for improvement in prescription patterns is underscored
Introduction
Frequent drug utilization review is necessary to provide knowledge of current drug use patterns necessary for improvement of prescribing habits and promotion of rational drug use [1]. While rational use of drugs involves optimal use of a well-documented drug at an affordable price in line with the patient’s clinical needs for an adequate period of time [1], drug utilization involves the prescription, dispensing, marketing, distribution and use of drugs in a society with the principal aim of facilitating their rational use [2].
A number of activities involving proper prescribing, dispensing and administration of medicines is needed among the healthcare team to ensure correct and effective use of medicines [3], with deviations in any or all of these resulting in medication error. Medication error can affect patient safety and quality of healthcare leading to prolonged hospitalization or even death [3]. Prescription error which is the most encountered medication error may be caused by many factors such as: polypharmacy, inadequate pharmacological knowledge of drugs, charts or documentation errors and inadequate pharmacological services, among others [4].
Infants and children constitute a large population in developing countries [5] and experts have shown that irrational prescribing and medication error have higher harm potential in children than in adults [6]. In hospital admissions, incidence of treatment error in children was reported to be as high as 1 in 6.4 orders with about 31 % resulting in pediatric death as against 13 % reported in adults [7,8]. The high incidence of death seen in children may be due to the fact that most medications used in the care of this group of patients are formulated and packaged primarily for adults and children may not be able to communicate effectively with providers [6]. Moreover, children’s renal, immune and hepatic functions are not well developed, thus creating pharmacokinetic and pharmacodynamic differences that predispose them to adverse drugs reactions and drug harm [6,9]. In view of these problems, there is need for good evidence-based prescribing to ensure appropriate use of drugs in patients and patient safety.
This study was carried out to evaluate the prescribing pattern and use of medicines in pediatric out-patient departments of two health facilities in Nigeria using the WHO prescribing indicators.
Methods
Study sites
This study was conducted in Anambra State, one of the states in the South-East geopolitical zones in Nigeria. Two referral hospitals, Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi and Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), Amaku, Awka were used.
NAUTH was established as a teaching hospital in 1990 with lots of annexes and its main centre is located at Nnewi, one of the big commercial centers in Anambra state. As the major tertiary hospital in the state, it serves as a referral centre and provides a wide range of medical and out-patient services to a population of > 30,990,559. One of the key departments of the institution is the pediatrics department with over seven subunits including general children out-patient clinic. The hospital has a total bed capacity of about 440, with 294 beds in the main hospital.
Formerly known as Anambra State University Teaching Hospital (ANSUTH), Awka, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), Amaku, Awka is located at the capital city of Anambra state. It serves as a referral centre for some medical conditions and has a pediatric department.
Study design and sampling
This study was a retrospective cross sectional study carried out in the pediatric out-patients department of NAUTH, Nnewi and COOUTH, Awka between May and June, 2015. Medical records of pediatric patients (aged 12 years or less) who attended the out-patient department of the hospitals between November 2014 and April 2015 were assessed.
A total of 750 prescriptions were randomly selected by picking at least 5 from every 10 prescriptions and these were used for the study. Data were collected using a designed form containing patients’ demographics, diagnoses, names of drugs and classes, dosage form, dose frequency, duration, route of administration as well as brand/generic name of the drug.
Ethical clearance
Full ethical approval (ref no. NUTH/CS/66/VOL.7/133) was obtained from the Ethical Review Board of Nnamdi Azikiwe University Teaching Hospital, Nnewi on July 9, 2015.
Data analysis
Data were evaluated using the WHO-developed prescribing indicators [1]. The WHO indicators calculated included: average number of drugs per encounter, percentage of drugs prescribed from generics, percentage of encounters with an antibiotic prescribed, percentage of encounter with an injection prescribed, and percentage of drugs prescribed from the National Essential Medicine List (EML). Analysis of data was carried out using Statistical Package for Social Sciences (SPSS) software version 20.0.
Results
Patients’ characteristics
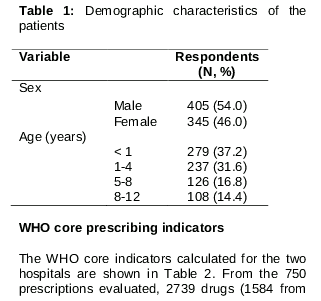
A total of 750 prescriptions (450 from NAUTH and 300 from COOUTH) were selected and used for the study. Descriptive statistics () showed more male than female admission in the two hospitals. The patient’s ages varied from a few months to 12 years, with majority aged 4 years or less (68.8 %) of age.
WHO core prescribing indicators
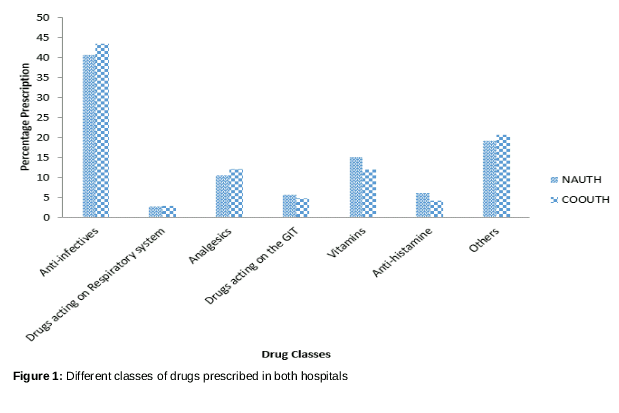
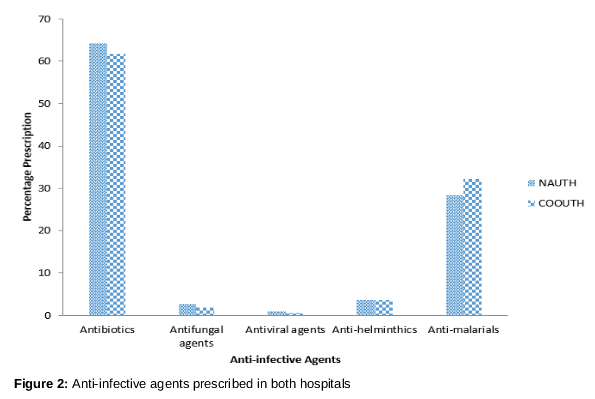
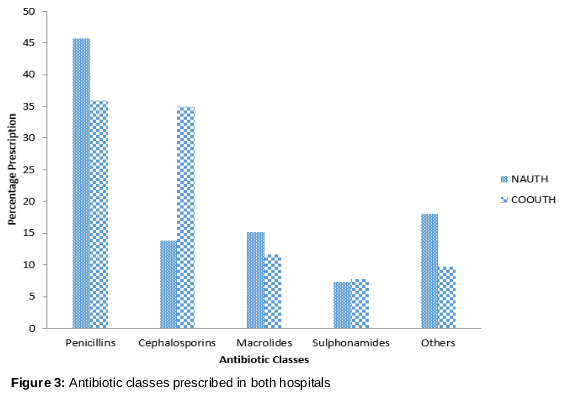
The WHO core indicators calculated for the two hospitals are shown in . From the 750 prescriptions evaluated, 2739 drugs (1584 from NAUTH and 1155 COOUTH) were prescribed. The average number of drugs per encounter in NAUTH and COOUTH were 3.5 ± 0.9 and 3.8 ± 1.1 respectively. The percentages of encounter with an antibiotic prescribed in both hospitals were similar: 77.1 % for NAUTH and 72.3 % for COOUTH. Most antibiotics were targeted at respiratory tract infections. The percentage of drugs prescribed by generic name was 65.3 % in NAUTH and 62.5 % in COOUTH. In NAUTH, 85.6 % of prescribed drugs were EML, which was similar to that of COOUTH (86.6 %). Injectable drugs prescribed per encounter were 10.2 % in NAUTH and 25.3 % in COOUTH. Most commonly prescribed drugs seen in both hospitals were anti-infectives with vitamins and analgesics also ranking high (). Among the anti-infectives, antibiotics were mostly prescribed followed by anti-malarials (), with the use of beta lactam antibiotics being common in both hospitals ().
Discussion
This study identified irrational use of drugs involving polypharmacy, high use of antibiotics and injectables and non-adherence to generic prescribing in pediatrics in the two hospitals studied. Rational prescribing is usually evaluated by conducting prescription audit at frequent intervals; the results of such studies are used to facilitate and promote rational drug use in health facilities [10]. Thus, the World Health Organization formulated a set of core drug use indicators that can be used to measure prescriber’s performance, patients experience at health facilities and the degree of effectiveness of the health personnel [11,12]. The indicators used for these assessments are prescribing indicators, patient care indicators, facility indicators and complementary indicators [13].
Polypharmacy is an important component of irrational prescribing. It implies the use of many drugs in one prescription or the prescription of too many medications for a particular patient with associated risk of drug interactions and adverse drug reactions [14]. It is known that the number and severity of adverse medication reactions are directly related to the number of drugs administered [6]. Thus, chances of polypharmacy occurring increase as the number of drugs in a prescription increases [15]. In the current study, the average number of drugs prescribed per encounter was 3.5 in NAUTH and 3.8 in COOUTH. These values are higher than the WHO recommended limit of not more than 2 drugs per encounter [16]. Consequently, the observed higher values are indicative of higher risk of polypharmacy in these hospitals. Similar results have been obtained in other studies in Nigeria and Pakistan [17,18]. The use of high number of drugs which may have been influenced by factors like financial incentives to prescribers by medical sales representatives and/or inadequate therapeutic training of prescribers can lead to high risk of drug interactions, adverse effects and high medication cost to the patients [19].
The percentage of antibiotics prescribed in the two hospitals is high compared to the WHO standard of 20.0 - 26.8 % [16]. This finding is comparable to other findings in some hospitals in Nigeria in which the percentage of antibiotics prescribed per encounter was within the range of 50 - 70 % [20-22]. This is similar to results from studies conducted in USA and Canada which showed that 50 and 85 % of antibiotics respectively, were prescribed inappropriately to children, with resultant increase in the cost of treatment, and adverse drug reactions [23]. The present study also observed that most of the antibiotics were targeted at respiratory tract infection and malaria with the Beta lactam antibiotics being the most prescribed. These observations are similar to the findings of Feudtuer et al who also expressed concerns over high use of antimicrobial and respiratory agents in pediatrics [24]. The high use of antimalarial agents found in the study is most likely due to the fact that children living in malaria endemic areas like Nigeria are vulnerable to frequent bouts of malaria attacks. WHO recommends that in promoting rational use of drugs, prescription of drugs should be in their international non-proprietary names [25]. The use of generic names results in low treatment cost and prevents errors and confusion in writing and dispensing prescriptions [26]. The percentage of drugs prescribed by generic name in the two hospitals was lower than the approved standard of 100 % [16]. Factors responsible for prescribing with brand names include promotional activities by companies, pressures from company representatives, lack of continuing education and training on rational prescribing principles and non-familiarity with generic names by most prescribers [27].
Although the percentage of drugs prescribed from the Essential Medical List (EML) was seen to be high in the two hospitals, they were still lower than the recommended value of 100 % [16]. This could be as a result of prescribers’ lack of awareness of the EML for children, or non-adherence to the list by some prescribers. A high incidence of unapproved use of drugs (prescribing outside the recommended dosage, indication, route of administration, or age of patient) and unlicensed use of drugs in the pediatric population has been reported [28]. A study conducted in the Europe and Australia indicated that 80 - 93 % of neonatal medications were off-labelled or unlicenced, with an overall off-label prescription rates of between 25 % and 60 % across populations and mostly seen in children less than 2 years of age and also in adolescents [29,30].
Finally, the study observed a high use of injections in COOUTH above the WHO acceptable standard of 10.1 - 17.0 % [31]. The observed irrational prescribing seen in these hospitals may predispose their patients to high risk of adverse drug effects and harm. Although most other studies have also reported similar findings, poor implementation of evidenced-based prescribing with poor training attitudes especially in developing countries has allowed this problem to persist. Education and training of prescribers with the introduction of prescription review systems and periodic audits have been suggested as ways of improving prescription practices [32]. These will help guarantee patients safety.
Conclusion
The results of this study indicate poor prescribing practices and irrational use of drugs in the two hospitals studied. While antibiotics are irrationally prescribed, polypharmacy which could lead to drug-drug interaction and adverse drug reaction is also evident in the hospitals. There is need for training and re-training of prescribers and healthcare professionals in general, to promote appropriate use of drugs, and thus, ensure patient safety.
References
Archives


News Updates